|
VICUS.COM (30 Aug. 2000)
-- A clinical advisory statement from the National Institutes of
Health, released in May, states that for middle-aged and older
patients, systolic blood pressure (the first and higher number in a
blood-pressure reading) is more important than diastolic pressure (the
second and lower number) for diagnosing and monitoring hypertension.
|
Fast
Facts: blood pressure
Blood pressure,
the force of the blood pushing against the walls of the
arteries, is expressed as a fraction. The
systolic pressure (top number) is the pressure of blood in the
vessels when the heart contracts; diastolic pressure (bottom
number) is the pressure of the blood between heartbeats when
the heart is at rest. High blood pressure is generally defined
as greater than 140/90.
When there is
no known cause of high blood pressure, it is called primary or
essential hypertension, which can be usually be controlled,
but not cured. High blood pressure traceable to a specific
cause is called secondary hypertension, which can usually be
cured if the cause is treated.
Source: National
Heart, Lung, and Blood Institute
|
To
understand why systolic blood pressure is important, it is necessary
to understand the physiology involved in transporting blood throughout
the body.
Blood circulates through
about 60,000 miles of blood vessels. Each heart beat pushes two to
three ounces of oxygenated blood from the heart into the aorta, the
body's largest blood vessel. From here, the blood flows to smaller
blood vessels and capillaries and eventually transfers its oxygen to
cells in the body.
The
force needed to circulate blood is called blood pressure and is
measured in millimeters of mercury (mm Hg). Normal blood pressure is
120/80 mm Hg. Systolic blood pressure (the higher number) is the
maximum force exerted against blood vessel walls each time the heart
beats, while diastolic blood pressure (the lower number) is the force
exerted on the blood vessels when the heart is resting between beats
(Zaret, Moser and Cohen, 1992).
The emphasis on diastolic
blood pressure in hypertension was based on early studies of young
people. Now we know that diastolic blood pressure rises until about
age 55 and then declines, while systolic blood pressure increases
steadily with age.
Therefore, it is possible
that many older people with "normal" diastolic blood
pressure are actually experiencing a worsening of the syndrome of
hypertension and its complications, including heart disease and stroke
(the first- and third-leading causes of death among Americans), kidney
damage, dementia and blindness (Kannel, 2000; Leonetti, et
al., 2000; Millar and Lever, 2000).
The
evidence for isolated systolic hypertension
When the systolic blood
pressure is high (at or above 140 mm Hg) but diastolic blood pressure
is less than 90 mm Hg, the condition is called "isolated systolic
hypertension," or ISH. In fact, for older Americans, ISH is a
common form of high blood pressure.
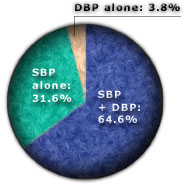
Among the more than 3,500
people (average age of 58 years; 55% women) participating in the
Framingham Heart Study, an ongoing epidemiological study that began in
1948, systolic blood pressure alone identified 96% of hypertensive
individuals. This percentage increases to 99% in people older than 60
years of age.
By comparison, diastolic blood pressure
correctly classified only 68.4% (Lloyd-Jones, et
al., 1999). The comparative ability to diagnose hypertension using
systolic or diastolic blood pressure alone or using both readings is
illustrated in the accompanying figure.
John
Russo Jr., PharmD, is senior vice president of medical
communications at Vicus.com. He is a pharmacist and medical writer
with more than 20 years of experience in medical education.

|
References:
Framingham Heart Study: http://www.americanheart.org/
Heart_and_Stroke_A_Z_Guide/fram..html
Kannel WB. Elevated systolic blood pressure as a cardiovascular
risk factor. Am J Cardiol. 2000 Jan 15;
85(2):251-5.
Kannel WB. The Framingham Study: Its 50-year legacy and future
promise. J Atheroscler Thromb. 2000; 6(2):60-6.
Leonetti G, Cuspidi C, et al. Is systolic pressure a
better target for antihypertensive treatment than diastolic pressure? J
Hypertens Suppl. 2000 Jul; 18(3):S13-20.
Lloyd-Jones DM, Evans JC, et al. Differential impact of
systolic and diastolic blood pressure level on JNC-VI staging. Joint
National Committee on Prevention, Detection, Evaluation, and Treatment
of High Blood Pressure. Hypertension. 1999 Sep;
34(3):381-5.
Millar JA, Lever AF. Excess mortality associated with increased
pulse pressure among middle-aged men and women is explained by high
systolic blood pressure. J Hypertens. 2000 Aug;
18(8):1155.
National Heart Lung and Blood Institute. NHLBI Issues New Clinical
Advisory On Systolic Blood Pressure. 4 May 2000.
http://www.nhlbi.nih.gov/new/press/may04-00.htm
Zaret BL, Moser M, Cohen LS [eds]. High Blood Pressure.
Chapter 12. Yale University School of Medicine Heart Book.
New York (NY): Hearst Books; 1992.
|


